Osteoma
From Wikipedia, the free encyclopedia
| Osteoma | |
|---|---|

Osteoma of external auditory meatus
|
|
| Classification and external resources | |
| Specialty | oncology |
| ICD-10 | D16 |
| ICD-9-CM | 213.0 |
| ICD-O | 9180/0, 9191/0, 9200/0 |
An osteoma (plural: "osteomata") is a new piece of bone usually growing on another piece of bone, typically the skull. It is a benign tumor.
When the bone tumor grows on other bone it is known as "homoplastic osteoma"; when it grows on other tissue it is called "heteroplastic osteoma".
Osteoma represents the most common benign neoplasm of the nose and paranasal sinuses. The cause of osteomata is uncertain, but commonly accepted theories propose embryologic, traumatic, or infectious causes. Osteomata are also found in Gardner's syndrome. Larger craniofacial osteomata may cause facial pain, headache, and infection due to obstructed nasofrontal ducts. Often, craniofacial osteoma presents itself through ocular signs and symptoms (such as proptosis).[1]
Contents
[hide]Variants
- "Osteoma cutis, but there is currently no way of detecting if and when this is likely to occur.
- "Fibro-osteoma"
- "Chondro-osteoma"
-
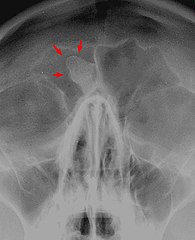
Osteoma of the frontal sinus seen on x-ray
-
Osteoma of the frontal sinus on CT
-
Osteoma


See also
References
- Michael S. Schwartz, MD; Dennis M. Crockett, MD. "Management of a Large Frontoethmoid Osteoma with Sinus Cranialization and Cranial Bone Graft Reconstruction".International Journal of Pediatric Otorhinolaryngology.
External links
- This page was last modified on 30 June 2016, at 00:48.
- Text is available under the Creative Commons Attribution-ShareAlike License; additional terms may apply. By using this site, you agree to the Terms of Use andPrivacy Policy. Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc., a non-profit organization.
Gardner's syndrome
From Wikipedia, the free encyclopedia
| Gardner syndrome | |
|---|---|
 |
|
| Classification and external resources | |
| OMIM | 175100 |
| DiseasesDB | 5094 |
| MedlinePlus | 000266 |
| eMedicine | med/2712 derm/163 |
| MeSH | D005736 |
| Orphanet | 79665 |
Gardner syndrome, also known as Gardner's syndrome or familial colorectal polyposis,[1] is an autosomaldominant form of polyposis characterized by the presence of multiple polyps in the colon together with tumors outside the colon.[2] The extracolonic tumors may include osteomas of the skull, thyroid cancer, epidermoid cysts,fibromas,[3] as well as the occurrence of desmoid tumors in approximately 15% of affected individuals.
Desmoid tumors are fibrous tumors which usually occur in the tissue covering the intestines and may be provoked by surgery to remove the colon. The countless polyps in the colon predispose to the development of colon cancer; if the colon is not removed, the chance of colon cancer is considered to be very significant. Polyps may also grow in the stomach, duodenum, spleen, kidneys, liver, mesentery and small bowel. In a small number of cases, polyps have also appeared in the cerebellum. Cancers related to Gardner syndrome commonly appear in the thyroid, liver and kidneys. The number of polyps increases with age, and hundreds to thousands of polyps can develop in the colon.
The syndrome was first described in 1951.[4] There is no cure at this time, and in its more advanced forms, it is considered a terminal diagnosis with a life expectancy of 35–45 years; treatments are surgery and palliative care, although some chemotherapy has been tried with limited success.
Contents
[hide]Genetics
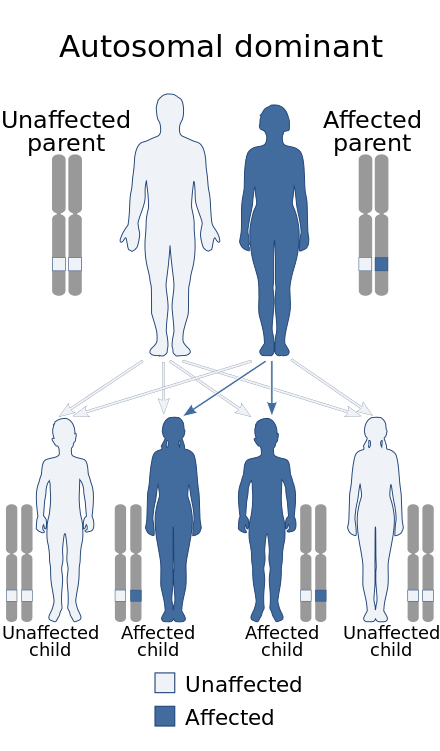
Gardner syndrome has an autosomal dominant pattern of inheritance.
Gardner syndrome is inherited in an autosomal dominant manner.[2] Typically, one parent has Gardner syndrome. Each of their children, male and female alike, are at 50% risk of inheriting the gene for Gardner syndrome.
Cause
Gardner syndrome is caused by mutation in the adenomatous polyposis coli (APC gene), located in chromosome 5q21 (band q21 on chromosome 5).[2] This gene is also mutant in familial adenomatous polyposis (FAP), a more common disease that also predisposes to colon cancer. Nuances in the understanding of genetics have caused some disorders to be split into multiple entities, while others merged into one genetic condition. After most of the second half of the 20th century, Gardner syndrome has been merged into FAP and is now considered simply a phenotypic subtype of FAP.[5]
Diagnosis
Gardner syndrome consists of adenomatous polyps of the gastrointestinal tract, desmoid tumours, osteomas, epidermoid cysts, lipomas, dental abnormalities and periampullary carcinomas. The incidence of the syndrome is 1:14,025 with an equal sex distribution. It is determined by the autosomal dominant familial polyposis coli gene (APC) on chromosome 5.[4]
Gardner syndrome can be identified based on oral findings, including multiple impacted and supernumerary teeth, multiple jaw osteomas which give a "cotton-wool" appearance to the jaws, as well as multiple odontomas, congenital hypertrophy of the retinal pigment epithelium (CHRPE), in addition to multiple adenomatous polyps of the colon. Gardner syndrome is also associated with familial adenomatous polyposis and may manifest as aggressive fibromatosis (desmoid tumors) of the retroperitoneum.[6]
Desmoid tumors arise most frequently from the aponeurosis of the rectus abdominal muscle of multiparous women. The extra-abdominal form is rare and desmoids of the breast may arise in the mammary gland or may occur as an extension of a lesion arising from the muscles of the chest wall. The incidence of mammary desmoid tumours is less than 0.2% of primary breast neoplasms. In Gardner’s syndrome the incidence ranges from 4% to 17%. Desmoid tumours associated with Gardner’s syndrome have been shown to have an alteration of the β-catenin pathway and over express β-catenin.[4]
Eponym
The syndrome is named for Eldon J. Gardner (1909–1989), a geneticist who first described it in 1951.[7]
See also
- Gorlin syndrome
- List of cutaneous conditions
- List of dental abnormalities associated with cutaneous conditions
- List of cutaneous neoplasms associated with systemic syndromes
References
- Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- Online 'Mendelian Inheritance in Man' (OMIM) 175100
- Luba MC, Bangs SA, Mohler AM, Stulberg DL (February 2003). "Common benign skin tumors". Am Fam Physician. 67 (4): 729–38. PMID 12613727.
- Rammohan A, Wood JJ (2012). "Desmoid tumour of the breast as a manifestation of Gardner's syndrome". Int J Surg Case Rep. 3 (5): 139–142.doi:10.1016/j.ijscr.2012.01.004. PMC 3312056
. PMID 22370045.
- "Gardner Syndrome". Cancer.net. American Society of Clinical Oncology. Retrieved 8 July 2016.
- DeVita. Cancer, Principles and Practice of Oncology, 8th Ed. p. 1742.
- Gardner EJ (June 1951). "A genetic and clinical study of intestinal polyposis, a predisposing factor for carcinoma of the colon and rectum". Am. J. Hum. Genet. 3 (2): 167–76. PMC 1716321
External links
- Gardner syndrome at NIH's Office of Rare Diseases
- Cancer.net Gardner Syndrome
- This page was last modified on 9 October 2016, at 00:34.
- Text is available under the Creative Commons Attribution-ShareAlike License; additional terms may apply. By using this site, you agree to the Terms of Use andPrivacy Policy. Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc., a non-profit organization.
Ann Med Health Sci Res. 2013 Jan-Mar; 3(1): 105–107.
PMCID: PMC3634204
Multiple Peripheral Osteomas of Forehead: Report of a Rare Case
This article has been cited by other articles in PMC.
Abstract
Osteoma is a benign slow growing osteogenic lesion, composed of well-differentiated mature bone tissue, characterized by the proliferation of compact or cancellous bone, almost exclusively found in the head and neck region. Central, peripheral and extra skeletal are the three variants of osteoma. Trauma, inflammation, developmental disorders and genetic defects are considered as the etiologic factors. Paranasal sinuses are the favourite locations of peripheral osteoma of the craniofacial region; frontal and ethmoidal sinuses being the common ones. Although, peripheral osteomas are usually benign, innocuous lesions, their size and prominent location on the visible parts of the face makes the surgical intervention necessary. We report case of multiple peripheral osteomas of forehead, without involvement of the frontal sinus, which is a rare variety.
Keywords: Asia, Osteoma of frontal bone, Osteomas, Peripheral osteoma
Introduction
Osteoma is a benign slow growing osteogenic lesion, characterized by the proliferation of compact or cancellous bone, almost exclusively found in the head and neck region. It can be of central, peripheral or extra skeletal variety.[1] Various concepts have been suggested for the aetiology of osteoma, but the exact factor still remains unclear. The peripheral osteoma arises by centrifugal growth from the periosteum, while central osteoma centripetally from the endosteum. They are seen commonly associated with the nose and the paranasal sinuses, the commonest being the frontal sinus. The incidence of osteoma of frontal bone and frontal sinus ranges from 37-80% in the reported cases.[2] But isolated cases of osteoma of the forehead, without involvement of the sinus, are rare.
We report here, a case of multiple peripheral osteoma of the frontal bone, without involvement of frontal sinus, causing a great deal of aesthetic concerns for the patient.
Case Report
A 39-year-old female patient reported with a complaint of facial asymmetry due to the presence of multiple swellings on the forehead. The swellings had been present for a period of around ten years. Patient didn’t give any specific history regarding the onset of the swelling. Patient noticed gradual increase in number and size of the swelling, since last three to four years. The swellings were not associated with a history of trauma or symptoms like pain, pressure sensation, paraesthesia and sinusitis. Only concern of the patient was related to the appearance.
On clinical examination, the patient appeared to be overall in good systemic health, except for the presence of the swellings, all the vital signs being within normal limits. Examination of the face revealed multiple, localized, oval shaped swellings on the forehead; located near the midline 3 cm above the glabella, the largest of which was of 4 × 4 mm in size [Figure 1]. The skin over the swelling was of normal in colour and texture, with no signs of ulcerations or scars. Similar, but smaller swellings were seen on the anterior portion of the scalp. The lesions were hard, non-tender and non-bleeding with smooth surface and diffuse margins. Fluctuancy, reducibility, compressibility and pulsatility were absent. The lesions were fixed to underlying bone, but overlying skin was pinchable. Regional lymph nodes were not involved.
39-year-old female with multiple bony hard swellings on the forehead (a) Frontal view (b) Lateral view
Lateral skull and lateral cephalometric projections were taken, which revealed localized areas of thickening of outer cortical table of frontal bone [Figure 2]. A computed tomography (CT) study of the head and neck revealed multiple lentiform hyper dense lesions involving the outer table of frontal bone [Figure 3]. The lesions appeared to be well defined and with its densities matching that of the osseous structure of the surrounding areas, it suggested the diagnosis to be a benign bony lesion. Based on the reported history, clinical and imaging findings we arrived at a diagnosis of multiple peripheral osteomas of frontal bone.
(a) Lateral cephalometric and (b) lateral skull projections showing localized areas of thickening of outer cortical table of frontal bone
CT image showing multiple lentiform hyper dense lesions involving the outer table of frontal bone (a) 3 dimensional view (b) Sagittal view
Surgical removal of the bony masses was done under general anesthesia and the specimen was sending for histopathologic examination. Patient reported with no symptoms on follow-up visit one month after the surgery [Figure 4].
Follow-up one month after the surgery (a) Frontal view (b) Lateral view
Discussion
Osteoma is a benign, osteogenic neoplasm composed of well-differentiated mature bone tissue, occurs due to proliferation of either compact or cancellous bone, usually an endosteal or periosteal location. Based on the location they can be of three types: Central (endosteal), peripheral (paraosteal, periosteal or exophytic) or extra skeletal (osseous choristoma);[1] the present case being a peripheral variety.
Many factors responsible for osteoma formation have been suggested, which include: Injury, inflammation, developmental disorders, genetic defects, Calcification of a polypus sinus, alteration of the calcium metabolism, metaplasia, and muscular theory.[3] But the exact pathogenesis of the osteoma has not been accurately explained. It has been suggested by many investigators that osteoma could be a reactive condition triggered by trauma, even minor that is unlikely to be remembered by the patient on a later date.[3] In the present case patient could not recall any trauma to that area.
Osteoma can arise at any age, but more frequently seen between the third and fifth decades. It has got a slight male predilection.[4] The case reported here is of a 39-year-old female. Paranasal sinuses are the favourite locations of peripheral osteoma of the craniofacial region, frontal and ethmoidal sinuses being the common ones. External auditory canal, orbit, temporal bone and pterygoid processes are the other locations.[5] The one reported here is a case of osteoma of the frontal bone without involvement of the sinus, which is very rare.
The tumour is often slow growing and asymptomatic, diagnosed incidentally on radiographs. But later on it can achieve a faster growth rate, as the rate of osteogenesis increases, and can cause deformation of the bone and compression of the adjacent structures. They usually appear as unilateral, sessile or pedunculated, well circumscribed, mushroom-like masses, ranging from 1.5 to 40 mm in diameter.[6] All these features are consistent with the present case, except the fact that the lesions are seen on either side of the midline.
Conventional radiographic imaging is generally sufficient to diagnose an osteoma. It appears as an oval, radiopaque, well-circumscribed mass attached by a broad base or pedicle to the host bone cortex. Usually, the osteoma does not exhibit any destruction of the surrounding bone.[7] In Computed Tomography image, osteoma appears as a smoothly demarcated, frequently lobulated, homogenously hyper dense mass. Better resolution and more precise localization are possible with CT scanning, especially with 3D reconstruction. CT scans are also help to rule out Gardner's syndrome, where multiple osteomas, impacted supernumerary teeth and odontomas may be present.[8] Since all the other features are not evident from CT scan, this case must be a nonsyndromic variety of multiple osteomas.
The differential diagnoses in this case include osteoid osteoma, dermoid cyst and lipoma. Although osteoid osteoma can be seen as a bony hard swelling of forehead, its painful nature helps in the exclusion.[9] Dermoid cyst and lipoma are also seen as subcutaneous nodules in the forehead; but they will be soft and fluctuant.[10]
There are three types of histologic variants for osteoma. They are compact or ivory type, cancellous, trabecular or spongy type and mixed type.[11] The recommended treatment is surgical excision. Recurrence is extremely rare and there are no reports of malignant transformation, which makes the treatment of asymptomatic lesions controversial.[12] In our patient surgical correction was done for cosmetic reasons. Patient reported with no symptoms and no sign of recurrence was revealed on follow-up visit one month after the surgery.
Conclusion
The peripheral osteomas are usually benign, innocuous lesions. However, their size and prominent location on the visible parts of the face can affect the appearance of a person and there by the quality of life, which necessitate the surgical interventions.
References
1. Sayan NB, Ucok C, Karasu HA, Gunhan O. Peripheral osteoma of the oral and maxillofacial region: A study of 35 new cases. J Oral Maxillofac Surg. 2002;60:1299–301. [PubMed]
2. Savastano M, Guarda-Nardini L, Marioni G, Staffieri A. The bicoronal approach for the treatment of a large frontal sinus osteoma: A technical note. Am J Otolaryngol. 2007;28:427–9.[PubMed]
3. Larrea-Oyarbide N, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Osteomas of the craniofacial region. Review of 106 cases. J Oral Pathol Med. 2008;37:38–42. [PubMed]
4. Wanyura H, Kamiński A, Stopa Z. Treatment of osteomas located between the anterior cranial base and the face. J Craniomaxillofac Surg. 2005;33:267–75. [PubMed]
5. Johann AC, de Freitas JB, de Aguiar MC, de Araújo NS, Mesquita RA. Peripheral osteoma of the mandible: Case report and review of the literature. J Craniomaxillofac Surg.2005;33:276–81. [PubMed]
6. Kerckhaert A, Wolvius E, van der Wal K, Oosterhuisa JW. Giant osteoma of the mandible: Case report. J Craniomaxillofac Surg. 2005;33:282–5. [PubMed]
7. Chandra J, Prasad BR, Veena KM. Osteoma of the frontal bone: A case report. J Clin Diagn Res. 2009;3:1426–30.
8. Castelino RL, Subhas BG, Shishir RS, Rao Kumuda Arvind HT. Multiple craniofacial osteomas: An isolated case. Arch Orofac Sci. 2011;6:32–6.
9. von Chamier G, Holl-Wieden A, Stenzel M, Raab P, Darge K, Girschick HJ, et al. Pitfalls in diagnostics of hip pain: Osteoid osteoma and osteoblastoma. Rheumatol Int. 2010;30:395–400.[PubMed]
10. Sewell LD, Adams DC, Marks VJ. Subcutaneous forehead nodules: Attention to the button osteoma and frontalis-associated lipoma. Dermatol Surg. 2008;34:791–8. [PubMed]
11. Rodriguez Y, Baena R, Rizzo S, Fiandrino G, Lupi S, Galioto S. Mandibular traumatic peripheral osteoma: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.2011;112:e44–8. [PubMed]
12. Longo F, Califano L, De Maria G, Ciccarelli R. Solitary osteoma of the mandibular ramus: Report of a case. J Oral Maxillofac Surg. 2001;59:698–700. [PubMed]
Articles from Annals of Medical and Health Sciences Research are provided here courtesy of Medknow Publications
http://ift.tt/2dmvv77



Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου